Introduction
From a structural perspective, the shoulder complex is two interrelated joint systems: the shoulder joint and the shoulder girdle. The shoulder complex needs the unified action of each system to provide both the expressive role and diverse functional requirements of the upper connection. As the shoulder joint is the most mobile joint in the body, the shoulder girdle is needed to anchor and stabilize the work of the arms and to transfer/ reciprocate force from the upper limbs to the spine/ core of the body.
Due to our contemporary patterns of cell phone use, computer use, driving, and general disconnection from the ground, as well as our psycho-emotional holding patterns and processes, our upper connection suffers. The shoulder complex is intimately related to the health of the neck and rest of the spine, our breathing quality, posture and alignment, and our connection with the world.
As movement educators, whether it be in yoga, dance, fitness, sport, somatics, martial arts, or recreation, helping our “movers” find stability, strength, and power in the upper connection is one of our challenges. To be confident in your program design, it is helpful to understand the joint actions, myofascial structures, and force-couple relationships in the shoulder complex. Our skill-set also includes the ability to guide experience through language, to cue effective movement at the shoulder, and to both ask for and provide feedback.
Quite a task! So let’s break this down, layering in one concept at a time. First, the bones and joints of the shoulder complex will be identified. Then, the joint actions of the shoulder complex will be discussed. Next, helpful myofascial considerations and relationships will be reviewed. The discussion will conclude with a method for applying the concepts presented.
Structural Kinesiology of the Shoulder Complex
Kinesiology is the study of movement, performance and function. The overlap of several sciences are found in kinesiology including anatomy, physiology, and biomechanics. Structural kinesiology has a specific focus on muscle, bones, and joints. With the current understanding of the neuromyofascial web, structural kinesiology helps us get a sense of the bony layer, the interaction of joints across the kinetic chain, and how this relates to myofascial slings or movement subsystems. When incorporating the structural principle of tensegrity into our movement training, one that recognizes compression in balance with tension, the components of structural kinesiology are viewed as interrelated parts in an ever adapting environment of forces.
Bones and Joints of the Shoulder Complex
The shoulder girdle surrounds the top of the axial skeleton like a cloak. The axial skeleton includes the bones of the skull, spinal column, rib cage, sacrum, and tailbone. The bones of the shoulder girdle include the right and left clavicle and the right and left scapula. Each clavicle articulates with the manubrium, the top bone of the sternum, anchoring the shoulder girdle to the axial skeleton.
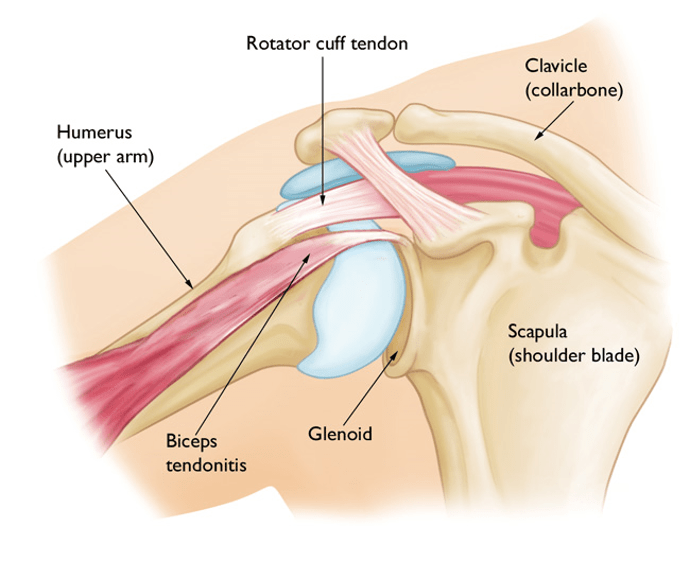
The glenohumeral joint, or the shoulder joint, is the articulation between the scapula and the humerus on each side of the body. The shoulder joint is a ball and socket joint with the head of the humerus moving within the shallow glenoid fossa of the scapula.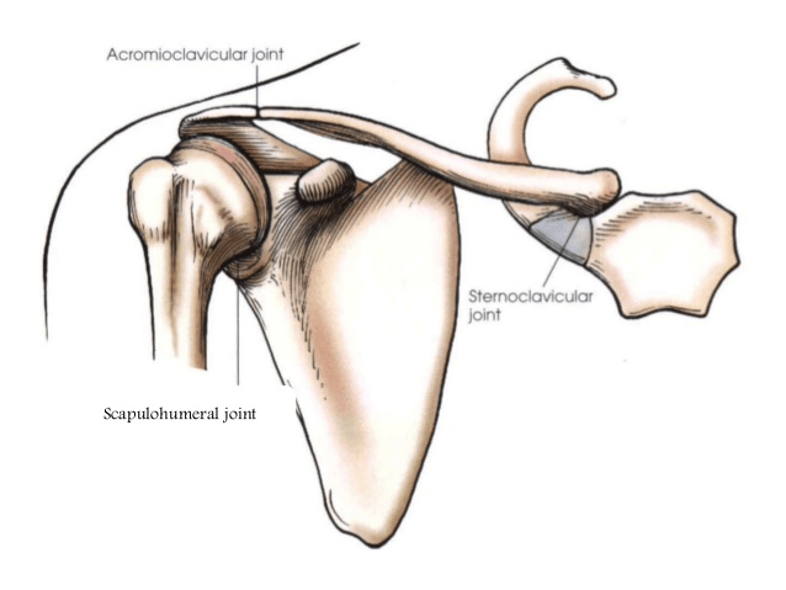
There are three joints to consider with the shoulder girdle: the sternoclavicular (joint between sternum and clavicle), the acromioclavicular (joint between the clavicle and acromion process of the scapula), and the scapulo-thoracic joint. The scapulo-thoracic joint is not a “true joint” but rather the translation or movement of the scapula on the thoracic spine.
The sternoclavicular and acromioclavicular joints have limited motion, yet these interrelated joint actions are incredibly important for healthy shoulder motion. With that said, as movement professionals, our work is mainly with the shoulder joint and the scapulo-thoracic joint. When these joints work well together, for the most part, so do the other joints of the shoulder complex.
Scapulohumeral Rhythm and the Joint Actions of the Shoulder Complex
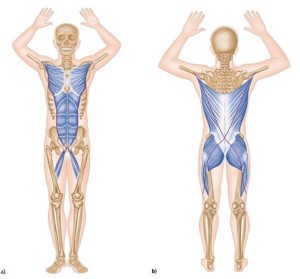
Scapulohumeral rhythm is the coordinated motion of the scapula and humerus during shoulder movement. Scapulohumeral rhythm describes the related joint motion between the glenohumeral and scapulo-thoracic joints. Some experts relay that the relationship has a 2:1 ratio so that for every 2 degrees of glenohumeral motion there is 1 degree of scapular motion. However, there can be quite a bit of individual variation and the ratio may change based on the movement task.
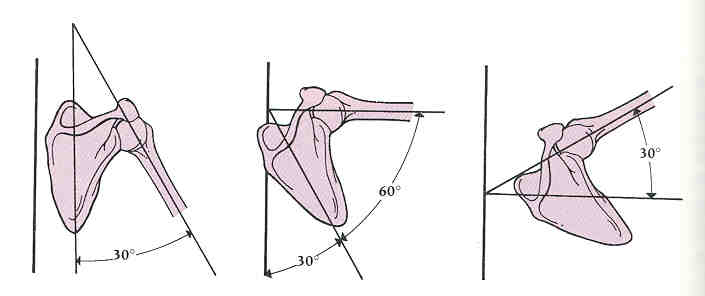
In the above image, we are seeing movement in the frontal plane: the scapular motion is upward rotation and the shoulder joint action is abduction. In each plane of motion, the joint actions of the shoulder girdle and the shoulder joint work together to allow for full range of motion. Above, if the scapula does not move properly when the arm moves into abduction then movement limitation and joint impingement may occur causing joint inflammation, tissue adhesion, and pain.
The shoulder joint moves in all planes of motion: abduction and adduction in the frontal plane; flexion and extension in the sagittal plane; internal and external rotation and horizontal abduction and horizontal adduction in the transverse plane. The ball and socket joint also allows for full circumduction or arm circling.
Scapular motion on the rib cage includes upward and downward rotation, elevation and depression, and retraction and protraction. The scapulae also have the tendency to tip. We commonly call anterior tipping (where the top of the scapula tips forward and the inferior angle pokes out) scapular winging.
Of course joints don’t move bones on their own, they are moved by muscle, stimulated by the nervous system, functionally influenced by the fascial net, which is in constant response to both the inner and outer environments through sensory feedback, hormones and unconscious processes. Obviously there are many factors we can discuss when looking at the influences of movement efficiency and coordination.
Keeping the scope within structural kinesiology presently, next we will take a look at several muscle synergies and myofascial considerations.
Scapular Stabilization
The stabilization systems of the shoulder complex give rise to the freedom of the upper connection. As parts to a greater whole, these stabilization systems support force transfer across the joint segments, through the arm, and into the central weave of the body.
Do you remember how the shoulder joint and shoulder girdle share a common bone – the scapula? And do you recall that the shoulder girdle actually attaches to the axial skeleton at the sternum via the sternoclavicular joint? Well, imagine managing a load in your right arm, say a grocery bag . . . how is it that the weight of the grocery bag doesn’t dangerously pull on the collar bone and separate it from the manubrium?
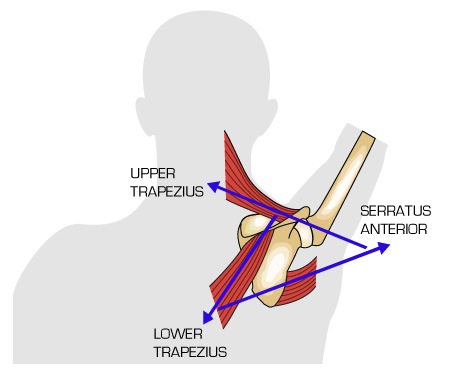
The answer is because of the scapulothoracic joint and its attachments to the back body via the scapular stabilizers. The muscular connection of the scapula to the thorax provides a foundation for the work of the arms and to the loads they negotiate. The five scapular stabilizers are pectoralis minor (the only one of the group that lies on the anterior aspect of the body), trapezius (upper, middle, and lower portions with separate innervations), rhomboids, levator scapulae, and serratus anterior. These scapular stabilizers arise from the axial skeleton and attach directly to the scapula.
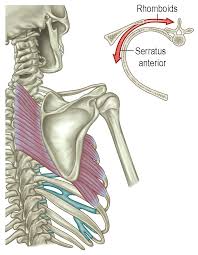 One primary relationship of the scapular stabilizers is between the rhomboids and serratus anterior. Rhomboids retract the shoulder blade while serratus anterior protracts the shoulder blade. Optimal muscle length-tension relationships between these two (yet fascially continuous) muscles promotes a balanced scapular position.
One primary relationship of the scapular stabilizers is between the rhomboids and serratus anterior. Rhomboids retract the shoulder blade while serratus anterior protracts the shoulder blade. Optimal muscle length-tension relationships between these two (yet fascially continuous) muscles promotes a balanced scapular position.
Along with this insight, let’s consider the force couple for promoting upward rotation of the shoulder blade. Remember that when the arm moves to the side, in shoulder abduction, the shoulder blade upwardly rotates. Three muscles synergistically create this motion: serratus anterior, upper trapezius, and lower trapezius.
Now consider a cue that is often given to enforce shoulder girdle stability in movement: keep the shoulder blades down and back. If the arms are moving overhead, and the cue is to keep the shoulder blades “down and back” there is a movement paradox at play.
The rhomboids will be called upon to keep the shoulder blades in retraction (moving toward the spine), yet the motion of the arms overhead requires some degree of protraction created by serratus anterior in scapular upward rotation. If serratus anterior is inhibited to shorten, because the rhomboids are keeping the shoulders “back”, then shoulder blade motion will be problematic and excessive elevation by the upper traps will need to occur to lift the arms. Or, alternatively, shoulder abduction will be forced without proper scapulohumeral rhythm and shoulder pain and possible joint damage can occur.
 The take away here is that there are intimate relationships between the muscles of the shoulder girdle (like the force-couple of upward rotation) to provide healthy shoulder joint mechanics. Additionally, there are myofascial considerations, like the fascial unity between the rhomboids and serratus anterior.
The take away here is that there are intimate relationships between the muscles of the shoulder girdle (like the force-couple of upward rotation) to provide healthy shoulder joint mechanics. Additionally, there are myofascial considerations, like the fascial unity between the rhomboids and serratus anterior.
A better cue when lifting the arms overhead may be to sense the shoulder blades moving like wings, spreading wide, and hugging the sides of the rib cage. Scapular stability will be enhanced and proper joint motion can occur with efficient scapulohumeral rhythm.
The concentric use of serratus anterior is important when either reaching out with the arms or when pushing away with the arms (like when pushing away from the ground or when pushing a box onto a high shelf or moving furniture across a room).
Shoulder Joint Stabilization
The glenohumeral joint has its own stabilization group that keeps the humeral head in the shallow glenoid fossa of the scapula. These four muscles, collectively called the rotator cuff muscles, have the acronym SITS: subscapularis, infraspinatus, teres minor, and supraspinatus. These muscles are also important for movement providing internal rotation, external rotation, and abduction. They are deep to the prime movers of the shoulder joint and key to healthy shoulder function.
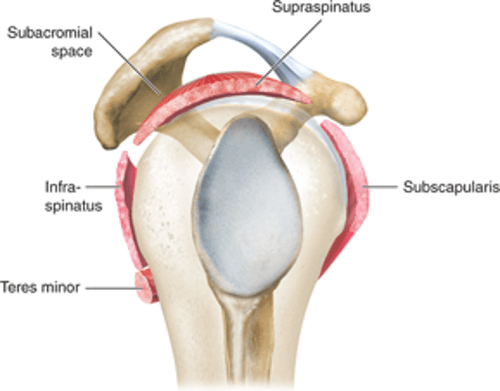 The side view of the glenoid fossa pictured here illustrates the rotator cuff muscles in relationship to the acromion, the scapular prominence that articulates with the clavicle in the shoulder girdle. The acromion is like a bridge under which passes the tendon of supraspinatus. The space between the two is called the subacromial space.
The side view of the glenoid fossa pictured here illustrates the rotator cuff muscles in relationship to the acromion, the scapular prominence that articulates with the clavicle in the shoulder girdle. The acromion is like a bridge under which passes the tendon of supraspinatus. The space between the two is called the subacromial space.
This space can become condensed with postural deviations like upper crossed syndrome, where resting postural position may include excessive joint actions like scapular elevation and/or anterior tipping and shoulder joint internal rotation. Excessive thoracic kyphosis and cervical extension are also common in this postural deviation.
When the subacromial space narrows, not only is the tendon of supraspinatus at risk for impingement, but also the tendon of the long head of the biceps brachii and the joint’s bursae (fluid filled sacs that act like lubricating cushions in the joint at specific places of friction).
 In terms of center directed motor programming, the joint stabilization system ideally comes online first, before the prime movers. When motor programming is altered, and the joint stabilization system is not adequately performing, the prime movers will have the double duty of stabilizing the joint and moving the joint through space. Prime movers are not suited for joint stabilization, so this strategy will eventually cause joint wear and tear.
In terms of center directed motor programming, the joint stabilization system ideally comes online first, before the prime movers. When motor programming is altered, and the joint stabilization system is not adequately performing, the prime movers will have the double duty of stabilizing the joint and moving the joint through space. Prime movers are not suited for joint stabilization, so this strategy will eventually cause joint wear and tear.
Prime Movers of the Shoulder Joint
So far we have discussed the shoulder girdle stabilizers (muscles that arise from the axial skeleton and attach to the scapula) and the shoulder joint stabilization system, or the rotator cuff (muscles from the scapula to the head of the humerus). The superficial muscular layer are the prime movers of the shoulder joint, which includes: latissimus dorsi, pectoralis major, and deltoid (anterior, medial, and lateral portions).
 The deltoid forms a shoulder “pad” surrounding the shoulder joint and rotator cuff muscles. The deltoid seemlessly merges with the trapezius across the bony station of the scapular spine and clavicle.
The deltoid forms a shoulder “pad” surrounding the shoulder joint and rotator cuff muscles. The deltoid seemlessly merges with the trapezius across the bony station of the scapular spine and clavicle.
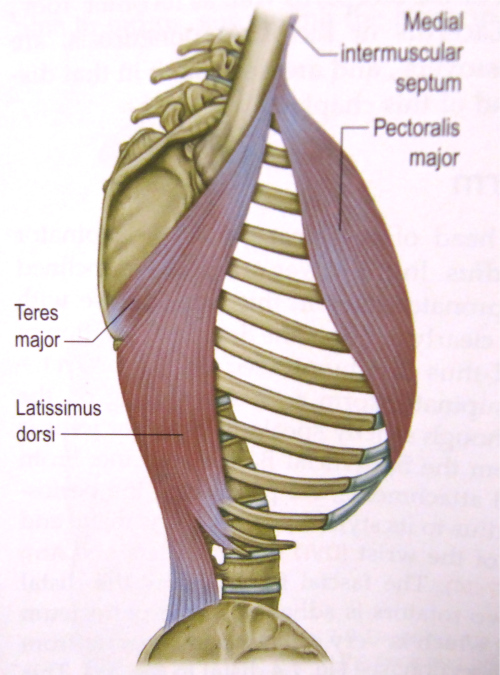
Pectoralis major and latissimus dorsi arise from the axial skeleton and commonly attach to the anterior aspect of the humerus under the deltoid at the intertubercular sulcus. The fascial continuity of pec major and latissimus dorsi indicates the influence these muscles have on the movement of the arm. The broad attachments of latissimus dorsi on the back body and pec major on the front body further illustrate their importance in powerful and athletic movement of the upper connection.
Additionally, the latissimus dorsi and pectoralis major are key contributors in two myofascial slings that link each arm to its opposite limb through the “core” of the body. These slings are the Functional Lines in Anatomy Trains and are also described as the Posterior Oblique Subsystem and Anterior Oblique Subsystem.
Functional Movement Subsystems
The two Functional Lines essentially link shoulder girdle to pelvic girdle across the body so that we may visualize an X on both the anterior and posterior body. Consider the contralateral organization of gait with the arms swinging in opposition to the legs. When the right arm is forward, at the moment of left heel strike we can imagine the anterior X: right pectoralis major passing to rectus abdominus and the obliques crossing the midline to the contralateral adductors.
 If we imagine the the left arm swinging back at the same moment when the right foot is in toe-off we have the posterior X: left latissimus dorsi feeding into the thoracolumbar fascia and crossing the midline to the contralateral gluteus maximus.
If we imagine the the left arm swinging back at the same moment when the right foot is in toe-off we have the posterior X: left latissimus dorsi feeding into the thoracolumbar fascia and crossing the midline to the contralateral gluteus maximus.
These myofascial slings describe four interrelated pathways that generate power and movement in the transverse plane. The coordinated action of the shoulder complex is influenced by the entire myofascial line.
Fascial restriction in any one of the four pathways will effect the function of the other pathways. For example, if the right anterior sling is restricted (functionally shortened) the left posterior sling will be functionally lengthened, potentially causing altered joint mechanics in the shoulder complex.
Push and Pull
One perspective of looking at movement from a functional lens is through the basic movement patterns. Basic movement patterns describe the primary movements utilized on a daily basis in order to successfully solve movement problems in our environment. Of the seven basic movement patterns, two seem worthwhile to mention here: upper body push and upper body pull.
Upper body push was mentioned earlier when discussing shoulder girdle upward rotation and is the action of pushing resistance away from the body or pushing the body away from the ground. Conversely, pulling resistance toward the body or pulling the body toward something promotes the action of upper body pull.
Each pattern has its own set of joint actions and muscle synergies. The joint actions in upper body push include shoulder girdle protraction and upward rotation and shoulder joint flexion, abduction, and horizontal adduction (think push-up) with elbow extension.
The joint actions in upper body pull include shoulder girdle retraction and downward rotation and shoulder joint extension, adduction, and horizontal abduction (think of pulling open a heavy door) with elbow flexion.
Muscles that concentrically contract in upper body push include the force couple for scapular upward rotation (serratus anterior, lower trapezius, upper trapezius) and pectoralis major, anterior deltoid, and the triceps.
Muscles that concentrically contract in upper body pull include the force couple for scapular downward rotation (pectoralis minor, rhomboids, levator scapulae) and latissimus dorsi, posterior deltoid, and the biceps.
Understanding these basic patterns can help with identifying effective language in cues and tracking support, sensation, and activation in movement practice.
Putting the Pieces Together
As movement professionals, we aim to help our students and clients find ease and efficiency in movement so that they can experience freedom in their lives to do what they want to do: play, recreate, and participate actively. When the deeper layers of the body are organized optimally, the superficial layers promoting global movement will respond accordingly. As the shoulder girdle is related to the spine and the movement of the pelvic girdle, it can be helpful to to consider the kinetic chain as a whole while also observing the function of the individual parts.
Taking into account the neuromyofascial web involves numerous processes, and often holding patterns live below conscious awareness, somatic inquiry seems to be an obvious place to begin. In the case of motor learning and repatterning, somatic inquiry influences autonomic tone, improves self awareness through sensory feedback, and provides tools for self-regulation.
As somatic inquiry is the experiential science of the personal consciousness, the opportunity for self-organization emerges and further learning is enhanced. Specific activation techniques and whole body integration exercises are well suited to follow felt-sense exploration as the body is in a “ripe” and ready state for applying new ideas in movement.
Interdisciplinary Movement & Somatics is my depth 250-hr teacher program for weaving somatic inquiry and movement science into 1:1 client programs. Movement assessments are part of this system as they provide insight to an individual’s habitual movement strategies. As sensory feedback is what initiates motor action, a somatic approach is central for cultivating intrinsic body support.
Wow, what a great article on the ghr! Incorporated anatomy trains and everything.
Thanks for the comment. So glad you found it useful!